Quack Finder: A Probabilistic Approach
Faisal Bukhari1, Mahrukh Saleem2, Rabia Zafar2, Muhammad Idrees1, Waheed Iqbal1, Zubair Nawaz1, and Saqib Saleem3
1Department of Data Science, University of the Punjab, Lahore, Pakistan
2Punjab University College of Information Technology, University of the Punjab, Lahore, Pakistan.
3Consultant Physician, Bahria International Hospital, Lahore, Pakistan.
* Correspondence: Muhammad Idrees Email: idrees@pucit.edu.pk.
Citation | Bukhari. F, Saleem. M, Zafar. R, Idrees. M, Iqbal. W, Zubair. N, Saleem. S, “Quack Finder: A Probabilistic Approach”. International Journal of Innovations in Science and Technology. Vol 4, Issue 2, 2022, pp:348-364
Received | March 25, 2022; Revised | April 08, 2022 Accepted | April 21, 2022; Published | April 23, 2022.
________________________________________________________________________
Quackery is profoundly rooted in rural areas, , but cities are also considerably affected. Countries, whether developed or developing, are experiencing this curse. Quackery is one of the primary reasons for the recent AIDS epidemic among children in Pakistan. In this research, we have conducted two separate surveys to study the causes of quackery. The sample sizes for the public and physicians were 157 and 58, respectively. The first questionnaire was handed to the respondents based in Pakistan to reveal the reasons behind the quackery and its widespread existence. The second questionnaire was designed to examine physicians' perceptions of quackery. The data were analyzed and we physicians having permit granted by the PMDC (Pakistan Medical and Dental Council) should be placed in doctor's clinics to help people distinguish between quacks and physicians. According to the conducted survey government may be held accountable behind the spread of quackery whereas lack of awareness from the media and high illiteracy rates are also the lead causes. Moreover, according to doctor’s perspective, awareness campaigns will surely help us to overcome this menace. It is not simple for common people to differentiate a quack from a doctor. To assist the common person, we have created a prototype android app called "Quack Finder"' based on our survey outcomes to predict whether an individual is a quack or a doctor.
Key-words: Quacks, Malpractice, Probabilistic approach, Self-medication, Android app.
Introduction
Quackery is growing daily, playing with citizens lives. It promotes fraudulent or ignorant medical procedures [1]. In2010, PHC (Punjab Health Care) Act defines a quack as a pretender providing health services without registering with the Pakistan Medical and Dental Council (PMDC), the National Council for Tibbs, the National Council for Homeopathy, and the Pakistan Nursing Council [2]. The history of quackery shows that doctors in the 15th century were very amateur, and herbalism was the medicine of that moment. A salve (containing mercury, which is a heavy toxic material) was produced by Paracelsus (then a doctor) and rubbed in a patient's rash so that the rash went away. Other physicians of that time claimed that the rash did not disappear but deepened into the patient's body and called it a quack for the use of "quacksalbe" (the German term for mercury, the element) [3]. A quack is a man who has learned specific methods by helping doctors or knowing the impact of particular drugs generally in a pharmacy or medical shop. We can easily find many hospitals around us run by dispensers, ward boys, and sanitary workers. The media disclosed that a fake neurosurgeon worked for eight months at Lahore Services Hospital [4]. More obviously, some quacks grumble reputable medical practitioners to run their clinics under their names, e.g., [5] reports, which show that qualified, licensed, professional doctors are the clinic's owners and not the Quacks. These include a restricted number of licensed professionals, or we can say workforce in health care systems [6]–[8]. Due to these reasons, individuals to consult quacks for their medical treatment because they promise to provide treatment at the least cost [9]. A sick person can compromise their child's education, but health is a commodity they must buy for their child, and because they can buy from a cheaper quack, they choose it [10]. Figure 1 demonstrates statistics on health care providers in Punjab, Pakistan, based on the PHC Anti-Quackery Strategy, June 2013.
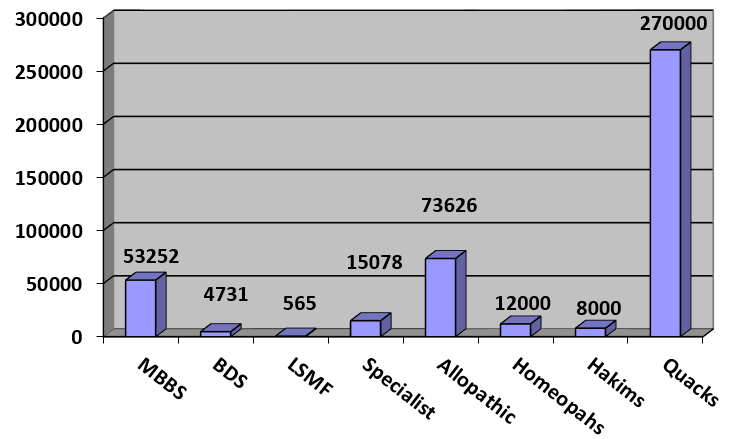
Figure 1: Health providers in Punjab, Pakistan [11].
This research aims to find out why ordinary people are compelled to go to quacks. We conducted two independent surveys with the general public and physicians to address this critical issue. We collected data from doctors based on different hospitals in Lahore, including Shaikh Zayed Hospital, Bahria Town Hospital, Fatima Memorial Hospital, Hameed Latif Hospital, Shaukat Khanum, Ittefaq Hospital, and Horizon Hospital. The main objectives of this research are as below,
- What are the reasons for the quacks' growth?
- What are the doctor's opinions to combat quackery?
- Is it possible to regulate quackery by displaying a PMDC certificate in a clinic?
- Whether or not quacks are allowed to exercise?
- A probabilistic android app to assist an individual in differentiating a quack from a physician.
The paper is organized as follows. Section 2 discusses the literature survey, Section 3 describes the material and the method used, and discusses the formulation of hypotheses. Section 4 includes a discussion of the results, including the outcomes of the hypotheses being tested. Finally, Section 5 concludes the paper.
Related Work
Quackery involves dishonest methods and argues that they are specialized in certain areas, typically medicine [1]. Quacks trap most rural and uneducated individuals living in urban areas to use their magic drugs [12], [13]. Quackery is the most significant issue in almost every country [1], [14], [15]. It is assumed that most illiterate and impoverished people are the target of quacks because most patients visit quacks because of their advertising and low prices, promising excellent treatment [16], [17]. In addition to these reasons, people are visiting quacks because of their commercialism, and in this era, commercialism overcomes professionalism [18]. More than 600,000 non-registered practitioners and 700,000 to 800,000 unqualified quacks were providing in Pakistan [19]. The U.S. Congress determined quackery to be massively dangerous consumer fraud against older adults [1]. All medical fields affect quackery, such as dentistry [20]–[22], homeopathy, and even dermatology [23]. The word denturism is used in some countries, and it seems to be a questionable practice [24] because they are practically outside their legal qualifications [21]. In the treatment of anal canal disease, quacks are more popular than qualified physicians due to their publicity in most countries such as India, Pakistan, and even in Europe and the Americas [12], [13], [16],[25].
People have faced several consequences because they are not aware of the healthcare industry, and quacks have put them on separate drugs without knowing the specific disease and without even understanding the aftereffects of their treatment. Thus, quacks play with people's life. According to Ain ul Momina et al.[26], the government's negligence has the biggest role in the spread of quackery. In [25], the factors play an important role in the growth of quacks and then further make an effort to distinguish between quackery and real medical practice. Thirty-two different causes of the increase in quackery were reported in [27], among which four were the most dominant ones. It includes a reluctance to seek professional advice and pay for professional services. In addition to it, the lack of punishments and monitoring of quacks was the major reason behind the widening of quackery. Sunita et al. [28] used an anonymous postal survey in India to determine the reasons of gap between patient-doctor relationship. Khan et al. [29] used a questionnaire-based survey. They discovered that about 65% of the dental quacks present in the urban area and 35% present in rural areas of Islamabad.. One possible way to cause hepatitis B, C, and HIV is through the community's fake dental procedures. The fight against quackery can minimize these infectious diseases [29]–[31].
Quacks are society's culprits because they have no clue what they will do with ordinary human beings by offering them their so-called new remedies. There must be some legislation for those who play with people's life [32]. Answer a query, "How do these fake dentists survive, and how does their training prosper?". Most of people replied to this query by stating that 70% of the Indian workforce comes from agricultural regions. Most of them are below the poverty limit, illiterate, less conscious, repeated appointments, and poor accessibility to actual physicians are factors for an increase in quackery [32]. The research was performed in India by the Association of Medical Consultants (AMC), according to which in 1998, there was about 1.5 million Quack against 0.6 million licensed allopathic professionals (Correspondent, 2002). To handle this issue, an Indian Supreme Court rit declared quacks' work illegal, and the Indian Medical Association (IMA) celebrated October 2 as "Anti Quackery Day" [33].
Similarly, the govt of Pakistan should propose some strict legislation against this curse. According to PMA, more than 600,000 quacks are active in the country, and they rise every day due to a lack of government checks and balances [34]. Khawaja Salman Rafiq (Chief Minister Punjab's Adviser on Health) said the government of Punjab would have to bring the rigorous measure against the quackery. Health Secretary Jawad Rafiq Malik said that a quacker would have to go to jail for five years, and Rs 0.1 million is fined according to the law. He further added that they would keep a check on the drug inspectors so that they would not think of providing any facility to quacks. In 2011, after inspecting 22,945 medical stores, 845 medical stores were closed [35]. One of the best methods to minimize the quacks percentage is to display the PMDC certification in clinics.
PMDC also supports and suggests that physicians show their registered PMDC certificates in their respective clinics (or practice places) [36]. According to PMDC authorities, only physicians with special medical or dental postgraduate skills can exercise as experts in their respective fields [36], [37]. PMDC has the authority to regulate medical negligence by physicians and dental quacks but is not accountable for other wellness professionals' fields (i.e., homeopaths, opticians, lady health workers, and quacks) [36]. For quacks, patients and their illegal activity fall out of their interest and judgment by forgetting professionalism [38], benefiting from the public trust. Their actions must be punished and classified as a crime [39]. Health professionals, governing bodies, institutes, law enforcement agencies, and the judiciary need to take urgent and robust steps [39].
Table 1. Literature Summary.
|
Paper |
Summary |
|
[15] |
In this paper, it is stated that most illiterate and impoverished people are the target of quacks because most patients visit quacks because of their advertising and low prices, promising excellent treatment. |
|
[17] |
The commercialization of quacks is the reason behind the growth of quackery. |
|
[26] |
The negligence of the government has the biggest role in the spread of quackery. |
|
[27] |
The reluctance to seek professional advice and to pay for the professional services. As well as the lack of punishments and monitoring of quacks was found to be the major reason behind the widening of quackery. |
|
[32] |
The poverty limit, illiterate, less conscious, repeated appointments, and poor accessibility to real physicians are all factors for an increase in quackery. |
Materials and Methods
We did two separate surveys, one from the public and one from the doctors. Online and face-to-face data collection methods have been used. We used Google Docs for the online survey and circulated questionnaires through emails, social networks, and other online means. The sample size for the public was 157, and the sample size for the doctors was 58. Data were divided into two communities, namely literate and illiterate while surveying the public.
The responses requested in the questionnaire show distinct concealed narratives about whether or not individuals are concerned about their physicians being skilled and whether or not their physicians are helpful. It reveals distinct parameters concerning people's perception of choosing their health providers, suspecting them as a quack, and still visiting them. It reveals the bitter truth about who is accountable for the presence of these so-called physicians in society, what actions to take to diminish them, and by whom. Opinions from Lahore's physicians have been drawn into account about the factors behind quackery, acts to fight quackery, and the part they can perform in controlling this social evil. After gathering information, we used statistical techniques and displayed outcomes, as shown in sections 4, 5, and 6, with the assistance of MATLAB, Google Docs, and Excel. In the survey findings, we used z-tests for testing the hypotheses depending upon the different proportions and p-values.
QuackFinder Android App
Based on our research findings, we have developed an android app called "QuackFinder," which could help people get to know and knock out these artists. The application's primary interfaces are extremely simple and are shown in Figure 10. This android application comprises nine questions; an equal rating was allocated to each based on the outcomes of the survey undertaken. After the answering all the nine questions in nine steps, the App will inform the use about the person in concern is a real doctor of a quack.
To use the App, first of all, the user needs to download the application, followed by the agreement to terms and conditions. After the approval, user has been asked the questions which are based on the findings i.e., the reasons which play an important role in distinguishing a quack from a doctor. These questions include e.g., how helpful a doctor is, to clarify the medical condition etc. Based on the answers given by the user, the application predicts a person to be a doctor or a quack.
Hypothesis Development
In order to understand the population point of view, we have stated some null and their respective alternative hypothesis [40], and these hypotheses are verified or tested using statistical techniques for finding their significance. For hypothesis testing, we assumed the level of significance traditionally called alpha "α" to be 0.05. Hypotheses are shown in Table 2.
Hypotheses' Testing: To test the above hypotheses, we used p-value testing of proportions. P-value is the statistical technique to identify the significance of the null hypothesis. Regardless of the method used for testing the hypothesis, whether it is a traditional method or a p-value test, each requires a test statistic. We used Z-test for testing the hypothesis based on the proportion (p= ) as shown in Equation 1.
Where, represents the population proportion of our claim, and p̂ represents the sample proportion. After finding the test statistic (Z), the value is used to find the area under the curve by using a table. After finding the p-value, we compared it with α in order to reject or accept our hypothesis. According to survey results shown in Table 2, it seems that H0A has an adequate proportion to state that the government is responsible for quackery in Lahore. H1B is accepted as most of the public thinks that the exhibition of the PMDC certificate is a way to eradicate quackery. During the survey, it was observed that some were neutral and gave us a reason which was stated as “Illiterate and even literate people cannot judge whether the certificate dispatched is fake or original, so how can quackery be stopped by taking this step.” H0C also has enough proportion to state that the public is in favor of ban quacks. They do not want them to continue their erroneous deeds. H0D is accepted; its test shows that people are compelled to go to quacks because qualified doctors have inordinate fee structures. H1E has a sufficient proportion, and it indicates that most people choose a doctor not because of his/her qualification but because of recommendations by their friends or relatives. It was described earlier that feedback from doctors from Lahore was also taken into consideration. From that feedback, we drew some hypotheses and tested them (Table 2). After testing, it is found that doctors are in favor of the PMDC certificate exhibition. H0F is accepted, and it reveals that from the doctor’s point of view, an exhibition of a PMDC certificate can cut down quackery. H0G is accepted after testing. Thus, it states that weak legislation against quacks is one of the significant reasons behind the increment in quackery. H0H and H0I have sufficient proportions. Thus, they are accepted and conclude that lack of awareness among messes encourages quacks to pursue the cruel acts that put the lives of patients at stake. It shows that by organizing awareness campaigns, quackery can be lessened, as shown in Table 2.
Experimental Results and Analysis
In Pakistan, quackery has strong roots since its independence. It is the most widely spreading curse. Fake doctors can be suicidal. This survey concludes many of the reasons behind its viral increase. Results from our survey clearly show that these so-called doctors exploit mostly illiterate and less-fortunate people because they do not bother to know whether the so-called healer, they are going to is qualified or not, irrespective of literate people. As shown in Figure 2, only 73.2% of literate people do care about the doctor they are visiting is qualified or not, whereas 86% of illiterate people are not concerned. That implies that mainly our illiterate fellows are promoting quackery.

Figure 2. Percentage of people who don’t care if their doctor is qualified or not.
Table 2. Hypotheses’ Analysis at α = 0.05 level of significance.
|
Hypothesis |
p-value |
Results |
|
H0A: P01 = 0.60 H1A: P01 > 0.60 |
0.060 |
Fail to reject null hypothesis i.e., H0A |
|
H0B: P02 = 0.75 H1B: P02 > 0.75 |
0.025 |
Accept the alternate hypothesis i.e., H1B |
|
H0C: P03 = 0.62 H1C: P03 > 0.62 |
0.060 |
Fail to reject null hypothesis i.e., H0C |
|
H0D: P04 = 0.65 H1D: P04 > 0.65 |
0.217 |
Fail to reject null hypothesis i.e., H0D |
|
H0E: P05 = 0.60 H1E: P05 > 0.60 |
0.022 |
Accept the alternate hypothesis i.e., H1E |
|
H0F: P06 = 0.95 H1F: P06 > 0.95 |
0.0008 |
Fail to reject null hypothesis i.e., H0F |
|
H0G: P07 = 0.90 H1G: P07 > 0.90 |
0.035 |
Fail to reject null hypothesis i.e., H0G |
|
H0H: P08 = 0.98 H1H: P08 > 0.98 |
0.0002 |
Fail to reject null hypothesis i.e., H0H |
|
H0I: P09 = 0.90 H1I: P09 > 0.90 |
0.0013 |
Fail to reject null hypothesis i.e., H0I |
P01: Proportion of the public who thinks the government is responsible for quackery.
P02: Proportion of the public who thinks by dispatching PMDC certificate by doctors, quackery can be diminished.
P03: Proportion of the public who thinks quackery should be banned.
P04: Proportion of the public who thinks inordinate expenses of doctors induce quackery.
P05: Proportion of the public who choose doctors recommended by friends/relatives.
P06: Proportion of doctors who imply that exhibiting PMDC certificate can curtail Quackery.
P07: Proportion of doctors who imply that inadequate legislation is responsible for the escalation of quacks.
P08: Proportion of doctors who imply that lack of awareness stimulates quacks to pursue their cruel act.
P09: Proportion of doctors who imply that quackery can be combated through awareness campaigns.
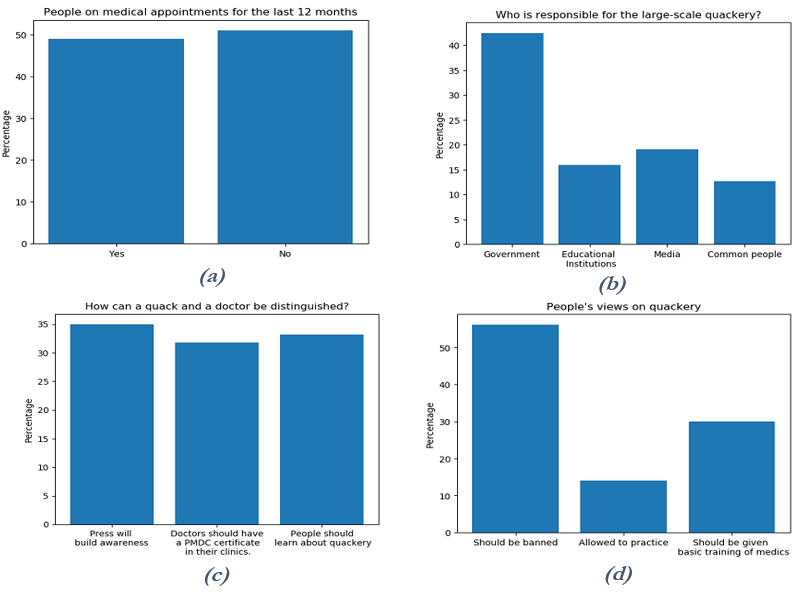
Figure 3. Public prospect of quackery. (a)People who have appointments with professional physicians over the previous 12 months (b) Who is liable for large scale quackery? (c) How to distinguish between a quack and a doctor? (d) People's views about quackery.
Figure 3(a) represents that the majority, 51% of people, do not take appointments from physicians over the previous 12 months. Figure 3(b) depicts that the majority, 52.4% of the
People of Pakistan, blamed the government for being responsible for quackery. Opinions of the people of Lahore were traced out to distinguish a doctor from a Quack. Opinions of the people of Lahore were traced out to distinguish a doctor from a Quack. According to the result shown in Figure 3(c), 35% population professes that media should create awareness about quackery. About 31.8% claim that doctor should display their certificates in clinics and people should be educated about the danger of quackery was the opinion articulated by 33.2% of the people. A majority of people, 56.1%, supported the idea of banning quackery. About 29.9% of the people were of the view that Quacks should be subject to training, and to the thinking of 14% of the people, they should be allowed to practice due to their lesser expenditures (Figure 3(d)).
The questionnaire upon study revealed that 40.1% and 38.2% of people find their doctors explaining their medical conditions to be very and moderately helpful, respectively, and 49% of the people have not been to a specialist for 12 months which clearly shows that they are not bothered by whether they are visiting a Quack, a general doctor, or a specialist. Figure 4 represents the majority of people think that a proper medical doctor clarifies medical conditions. Many anti-quackery strategies have been made, but more than 80% of people think due to the weak legislation depicted in Figure 5, no change has occurred regarding this menace. The media was held liable for quackery by 19% of the people and15% and 12% of the people blame educational institutions and themselves, respectively, for this persistent growth of quackery (Figure 5). 88% of the people claimed lack of awareness is the leading cause of quackery (Figure 5).
The community of Lahore, narrated different reasons for choosing a physician. The answers unfold that none of the single parameters is ascendant of the other. Figure 6 illustrates that 52% of the community prefer doctors suggested by their friends/relatives, 40% due to vast clientele of doctors, 41% voted for those who are near to their house, 40% choose due to their qualification and 21.7% due to the advertisements being shown. However, doctors suggested by friends or relatives still possess the highest percentage. Nowadays, medical quackery is influencing people to fall for it. We questioned some of the reasons one can come up with a person to be a Quack (Figure 7). The result shows that 27% of people comprehend their practitioner as Quack when he says that all the patient's symptoms are in their mind. 41% of people visualize quacks when they put them on medication for a long time. About 38% notified them to be a Quack when they did not tell patients about their disease, and 29% suspect quacks for not having excellent communication skills and 35% for not displaying PMDC certificates in clinics.
We observed why people continue visiting quacks, knowing them to be a pretender as it is visible in Figure 3 that approximately 9% of people find their health providers to be slightly helpful and 2% not at all useful but still prefer the same doctor. We stated some reasons behind this reality shown in Figure 8. According to result, 62% of the people agree that they choose quacks because their lower expenditures captivate them. Insufficiency of medical facilities compels people to seek help from quacks, which is the reason stated by 17% of the population of Lahore and clarifies that this reason does not play an essential part in promoting quackery. About 21% of victims say that they are inclined to a Quack because their medicine grants quick recovery. Even though these so-called healers might give them steroids which can lead to severe disorders and even be deadly. About 19% of people choose quacks because medicines prescribed by them have no side effects. People, in the beginning, think they are not having any reactions or aftereffects, but continuous treatment from a Quack may lead to severe disorders. About 6% of people have deep faith in them as they might be promising them a quick and miraculous recovery, but eventually, it might be injurious.
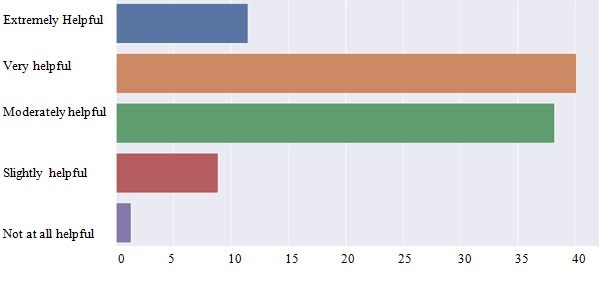
Figure 4. Public prospect of quackery. How helpful the doctor is to clarify the medical conditions?
Doctor’s Perception
The questionnaire was handed over to many doctors of Lahore in order to determine the reasons behind quackery. According to the doctor’s perceptions, 82% and 90% of the doctors correspond to the reasons that weak legislation and lack of awareness/education are the leading cause of quackery, respectively. These reasons comprise the highest percentage, among others. About 53% of health providers declared TV/media to be responsible for this curse. About 66% claim that an increase in population is the reason. As stated by 60% of doctors, overpriced fee structure by specialists is the leading cause of quackery, and quacks bribing government officials is the reason reported by 64% of the doctors (Figure 8). The questionnaire for doctors included another portion to uncover ways to combat quackery. Awareness campaigns are the most rated by most (84%) way to battle against quackery. Two reasons constituting the second-highest percentage are a ban on Quack commercials and enforcement of anti-quackery laws. These two reasons have the same proportion, which is 82%. Free medical camps by doctors and the opening of medical colleges in small cities can be ways to stand against quackery, claimed by 60% of the doctors of Lahore (Figure 8). Displaying PMDC certificates in clinics can control quackery as per claim by88% of the doctors. About 96% of doctors strictly condemned quacks and were of the view that they should not be provided with any training to practice and should be banned entirely (Figure 9(a) & Figure 9(b)).

Figure 5. Public prospect of quackery. What are the triggers of quackery?

Figure 6. Public prospect of quackery. What are the parameters to choose a doctor?
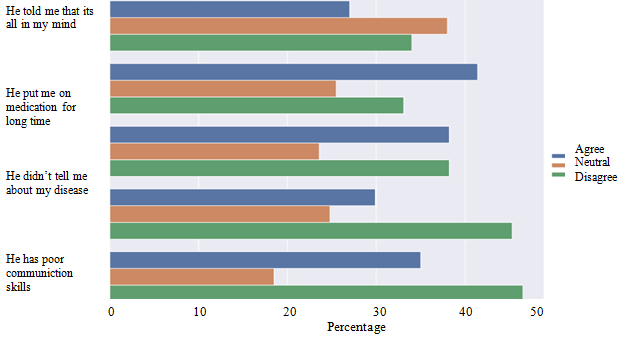
Figure 7. Public prospect of quackery. What signs cause you to doubt that a doctor is a quack.

Figure 8. Doctors’ perspective. How can we abolish quackery?

Figure 9. Doctors' perspective. (a) Do train quacks. (b) Does PMDC certificate display in clinics.
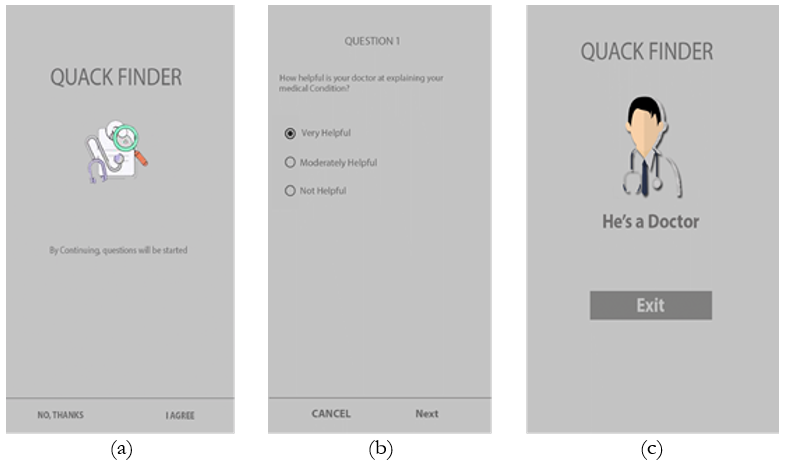
Figure 10. Output interface of android application. (a) Home screen (b) Questions interface (c) Result interface.
Conclusion
This research clearly shows that quacks have enjoyed dominance in Pakistan for countless years. These pretenders have already felt deprivation and hardship among individuals and take complete advantage of it. Several reasons have been given for the alarming increase in the population targeted by quacks. Our study concluded that these unqualified practitioners target mostly illiterate and underprivileged people. People are satisfied with their medical practitioners, regardless of their knowledge of being a quack or a qualified doctor. Most of the people in Lahore, after being questioned, have revealed that they have not been a medical specialist for a year. The government has failed to raise awareness of this social evil. Many quackery elimination strategies have been implemented but are not vigorously enforced. People here mostly prefer the doctors suggested by their friends/relatives. A practitioner who puts people on a medicine roller coaster, which is not providing any relief, is the one most suspicious to be a Quack. However, people are lucky enough to still visit these quacks mainly because of their lower fees. Our findings suggest that media, education, and physicians (by displaying their PMDC certificates) could help ordinary men to distinguish a quack. Most individuals have strictly condemned quackery, but some percent have suggested that these quacks should be trained to practice because of their low fees. In the opinion of the physicians, lack of education/awareness and weak legislation are the two main reasons for quackery. Most of them suggest that maintaining a reasonable fee structure and enforcement of anti-quake laws may not be the only means of facilitating people. Ban on Quack commercials and awareness campaigns should be upheld. Doctors argued that it should be prohibited entirely to display PMDC certificates in clinics to control quackery. The app used for probabilistic verification of the doctor is implemented, and its interfaces are given in
Figure 10.
References
[1] W. T. Jarvis, “Quackery: a national scandal - ” Clinical chemistry, vol. 38, no. 8, pp. 1574–1586, 1992. https://pubmed.ncbi.nlm.nih.gov/1643742/.
[2] “Quackery - Wikipedia.” https://en.wikipedia.org/wiki/Quackery.
[3] “M. Wellness, “The history of quackery,” 2009.” https://phc.org.pk/downloads.aspx.
[4] A. Mehmood “Fake neurosurgeon worked at Lahore’s Services Hospital for eight months - Pakistan - DAWN.COM.” https://www.dawn.com/news/1252234.
[5] William T. Jarvis, Ph.D “Why Health Professionals Become Quacks | Quackwatch. December 11, 1998” https://quackwatch.org/related/quackpro/ .
[6] M. I. Roemer, “Health manpower allocation in developing countries.,” Asia. Pac. J. Public Health, vol. 1, no. 1, pp. 20–24, Jul. 1987, doi: 10.1177/101053958700100107.
[7] A. Ahmed and M. Ahmed “The Telemedicine Landscape in Pakistan- Why are we falling behind? - PubMed.” The Journal of the Pakistan Medical Association, vol. 68, no. 12, pp. 1820– 1822, 2018. https://pubmed.ncbi.nlm.nih.gov/30504948/ .
[8] P. Mannava, A. Abdullah, C. James, R. Dodd, and P. L. Annear, “Health systems and noncommunicable diseases in the Asia-Pacific region: a review of the published literature,” Asia-Pacific J. public Heal., vol. 27, no. 2, pp. NP1–NP19, Mar. 2015, doi: 10.1177/1010539513500336.
[9] S. H. Short, “Health quackery: Our role as professionals,” J. Am. Diet. Assoc., vol. 94, no. 6, pp. 607–611, 1994, doi: 10.1016/0002-8223(94)90154-6.
[10] “H. Ahmed, “Noisy quacks under the knife,” 2015 | Pakistan Today.” https://archive.pakistantoday.com.pk/2015/06/06/city/lahore/noisyquacks-under-the-knife/.
[11] T. H. E. Punjab and H. Commission, “The Punjab Healthcare Commission Act 2010 (Act XVI of 2010) Healthcare Commission and Governance,” 2010.
[12] R. Datta, “The World of Quacks: A Parallel Health Care System in Rural West Bengal,” IOSR J. Humanit. Soc. Sci., vol. 14, no. 2, pp. 44–53, 2013, doi: 10.9790/0837-1424453.
[13] S. Barrett “Health frauds and quackery - PubMed.” FDA consumer, vol. 11, no. 9, p. 12, 1977 https://pubmed.ncbi.nlm.nih.gov/10305004/ .
[14] by C. J S Thompson, G. de Francesco, and E. Jameson, “Health for sale: quackery in England, 1660–1850,” Med. Hist., vol. 36, no. 1, p. 91, Jan. 1992, doi: 10.1017/S0025727300054673.
[15] N. P. Taschner “Brazilian Cancer Quackery - Document - Gale Academic OneFile.” Skeptic (Altadena, CA), vol. 23, no. 1, pp. 8–12, 2018. https://go.gale.com/ps/i.do?id=GALE%7CA535101648&sid=googleScholar&v=2.1&it=r&linkaccess=abs&issn=10639330&p=AONE&sw=w&userGroupName=anon~40aee12c.
[16] P. J. Gupta, “The role of quacks in the practice of proctology,” Eur. Rev. Med. Pharmacol. Sci., vol. 14, no. 9, pp. 795–798, 2010.
[17] N. Sheth and P. A. Nair, “Contact Dermatitis Due to Quackery,” Indian J. Dermatol., vol. 62, no. 6, p. 669, Nov. 2017, doi: 10.4103/IJD.IJD_459_17.
[18] W. T. Jarvis, “QUACKERY: THE NATIONAL COUNCIL AGAINST HEALTH FRAUD PERSPECTIVE,” Rheum. Dis. Clin., vol. 25, no. 4, pp. 805–814, Nov. 1999, doi: 10.1016/S0889-857X(05)70101-0.
[19] M. S. Rana et al., “Potential impact of COVID-19 pandemic on escalating antimicrobial resistance in Pakistan,” J. Infect., vol. 83, no. 3, pp. e12–e13, Sep. 2021, doi: 10.1016/J.JINF.2021.07.024.
[20] A. Jain, “Dental quackery in India: an insight on malpractices and measures to tackle them,” Br. Dent. J. 2019 2264, vol. 226, no. 4, pp. 257–259, Feb. 2019, doi: 10.1038/s41415-019-0014-3.
[21] D. W. Chambers, “Quackery and fraud: understanding the ethical issues and responding.,” J. Am. Coll. Dent., vol. 70, no. 3, pp. 9–17, 2003.
[22] U. Kalidhar and A. Kaur, “Research Journal of Pharmaceutical , Biological and Chemical Sciences REVIEW ARTICLE,” Res. J. Pharm. Biol. Chem. Sci., vol. 2, no. 1, pp. 1091–1106, 2013.
[23] T. T. Perls, “Anti-aging quackery: human growth hormone and tricks of the trade--more dangerous than ever,” J. Gerontol. A. Biol. Sci. Med. Sci., vol. 59, no. 7, pp. B682–B691, Jul. 2004, doi: 10.1093/GERONA/59.7.B682.
[24] D. Bennadi and V. Konekeri “Quackery, fraud, and denturists.” Research Journal of Pharmaceutical Biological and Chemical Sciences, vol. 6, no. 2, pp. 504–509, 2015 https://www.researchgate.net/publication/8687279_Quackery_fraud_and_denturists
[25] M. J. Mehlman, “Quackery,” Am. J. Law Med., vol. 31, no. 2–3, pp. 349–363, 2005, doi: 10.1177/009885880503100209.
[26] A. U. Momina and R. Zakar, “Implementation of the Anti-Quackery Mandate Punjab Healthcare Commission: Challenges and Limitations,” Pakistan J. Med. Heal. Sci., vol. 15, no. 9, pp. 2150–2153, Sep. 2021, doi: 10.53350/PJMHS211592150.
[27] J. O. Dada and G. O. Bamigboye, “Diagnosing the Causes of Quackery in Quantity Surveying Practice in Lagos State, Nigeria,” J. Constr. Bus. Manag., vol. 5, no. 1, pp. 28–37, Jul. 2021, doi: 10.15641/JCBM.5.1.950.
[28] S. S. Kurpad, T. Machado, and R. B. Galgali, “Is there an elephant in the room? Boundary violations in the doctor-patient relationship in India,” Indian J. Med. Ethics, vol. 7, no. 2, pp. 76–81, 2010, doi: 10.20529/IJME.2010.029.
[29] A. S. Khan, A. Syed, A. Qureshi, S. Ijaz, and A. A. Khan, “Evaluation of problems reated to malpractice and professionalism in Islamabad area- A study,” Pak Oral Dent J, vol. 24, no. 1, pp. 74–6, 2004.
[30] A. Fatima Asif, “Appraisal of National Response to Chronic Hepatitis in Pakistan,” J. Islam. Med. Dent. Coll., vol. 8, no. 1, pp. 3–7, 2019, doi: 10.35787/jimdc.v8i1.301.
[31] C. Break et al., “in Dentistry in Dentistry,” no. December, pp. 1–3, 2012, doi: 10.4103/bjhs.bjhs.
[32] A. Online, I. Journal, and R. Scientific, “BEWARE OF QUACKERY : UNQUALIFIED DENTAL PRACTICE IN INDIA How To Tackle Quackery ?,” vol. 6, pp. 3428–3430, 2015.
[33] T. K. Das, “Quack: Their Role in Health Sector,” SSRN Electron. J., no. October 2008, 2011, doi: 10.2139/ssrn.1292712.
[34] “Anti-Quackery Drive Kicks Off in Karachi.” https://www.dentalnewspk.com/30-Jan-2019/anti-quackery-drive-kicks-off-in-karachi.
[35] N. source, “Lahore: 5,620 medical stores outlets of quacks sealed.” https://www.thenews.com.pk/print/371402-vip-guest-house.
[36] “T. P. H. Commission, “PHC anti quackery strategy 2013” https://www.phc.org.pk/antiquackeryStrategy.aspx.
[37] Shazy “Checking quackery : PMDC to move against unapproved colleges | PFMSG FORUM.” https://forum.pfmsg.com/threads/checking-quackery-pmdc-to-move-against-unapproved-colleges.2457/.
[38] E. J. Latessa, F. T. Cullen, and P. Gendreau, “Beyond correctional quackery - Professionalism and the possibility of effective treatment,” Fed. Probat., vol. 66, no. 2, pp. 43–49, 2002.
[39] I. Ulhaq and N. H. Service, “Medical Malpractice in Pakistan ;,” no. May, 2016, doi: 10.17957/TPMJ/16.2923.
[40] R. R. Wilcox, “Introduction to Robust Estimation and Hypothesis Testing,” Introd. to Robust Estim. Hypothesis Test., 2012, doi: 10.1016/C2010-0-67044-1.
 |
Copyright © by authors and 50Sea. This work is licensed under Creative Commons Attribution 4.0 International License. |